
University Hospital Regensburg, Germany. Department of Trauma Surgery
Lateral tibial plateau fracture left tibia, type Schatzker V
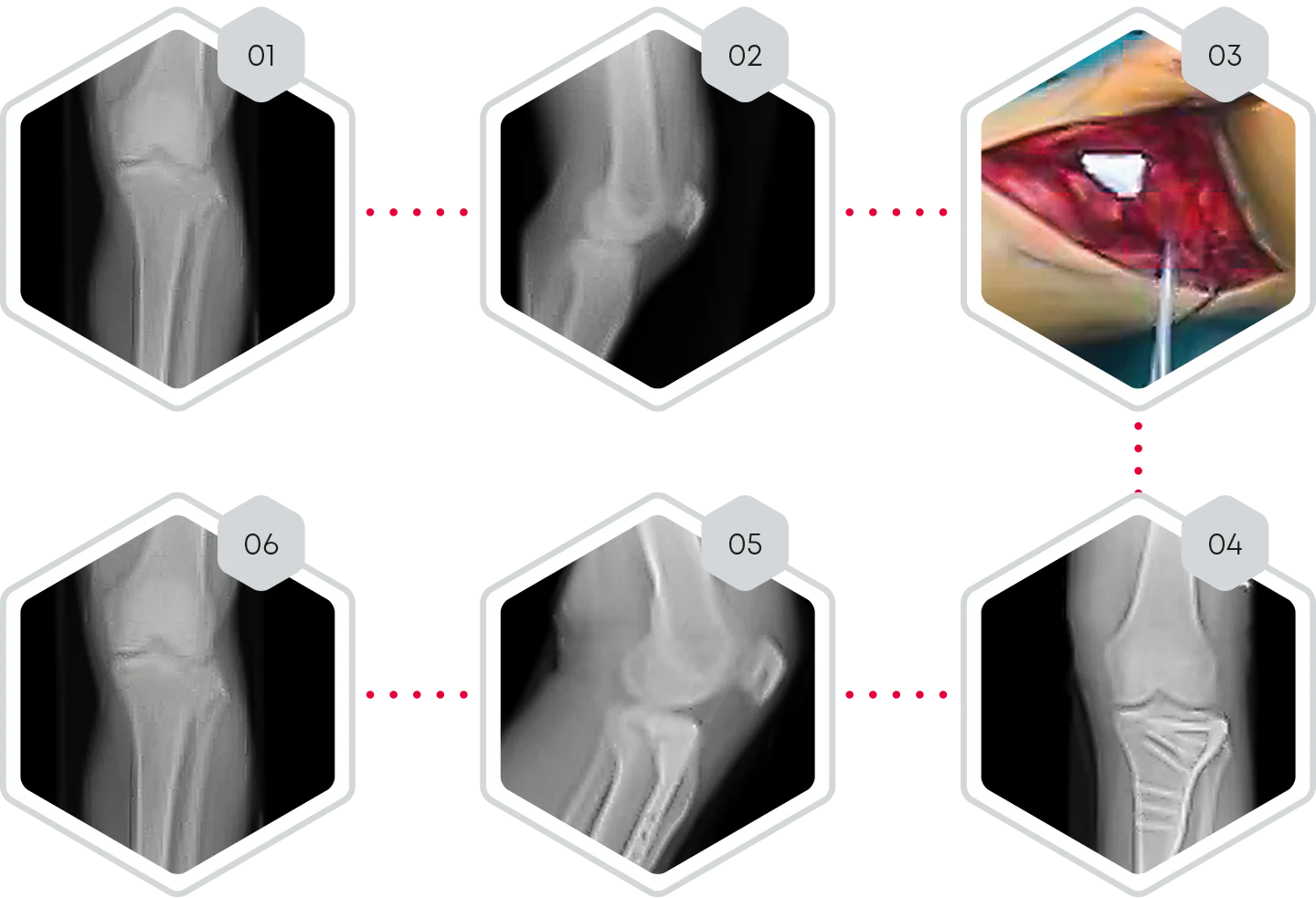
❯ 01-02 Pre-operative X-rays of tibial plateau fracture, type Schatzker V
❯ 03 Open reduction of lateral tibial plateau left and bone defect filling with CERASORB® CPC
❯ 04-05 Day 1 post-operative x-rays.
❯ 06 6 months post-operative x-rays.
❯ Clinical follow-up.
❯ CERASORB® CPC was easy to handle during the operation and allowed sufficient bone defect filling.
❯ 6 months post-operative, X-rays showed complete fracture healing with osseous integration and initial degradation of CERASORB® CPC. No subsidence of the articular surface could be observed.
❯ CERASORB® CPC supports the defect through good osseous integration and is gradually replaced by the newly formed bone.
University Hospital Regensburg, Germany. Department of Trauma Surgery
Ankle fracture type WEBER C with bony defect of distal fibula
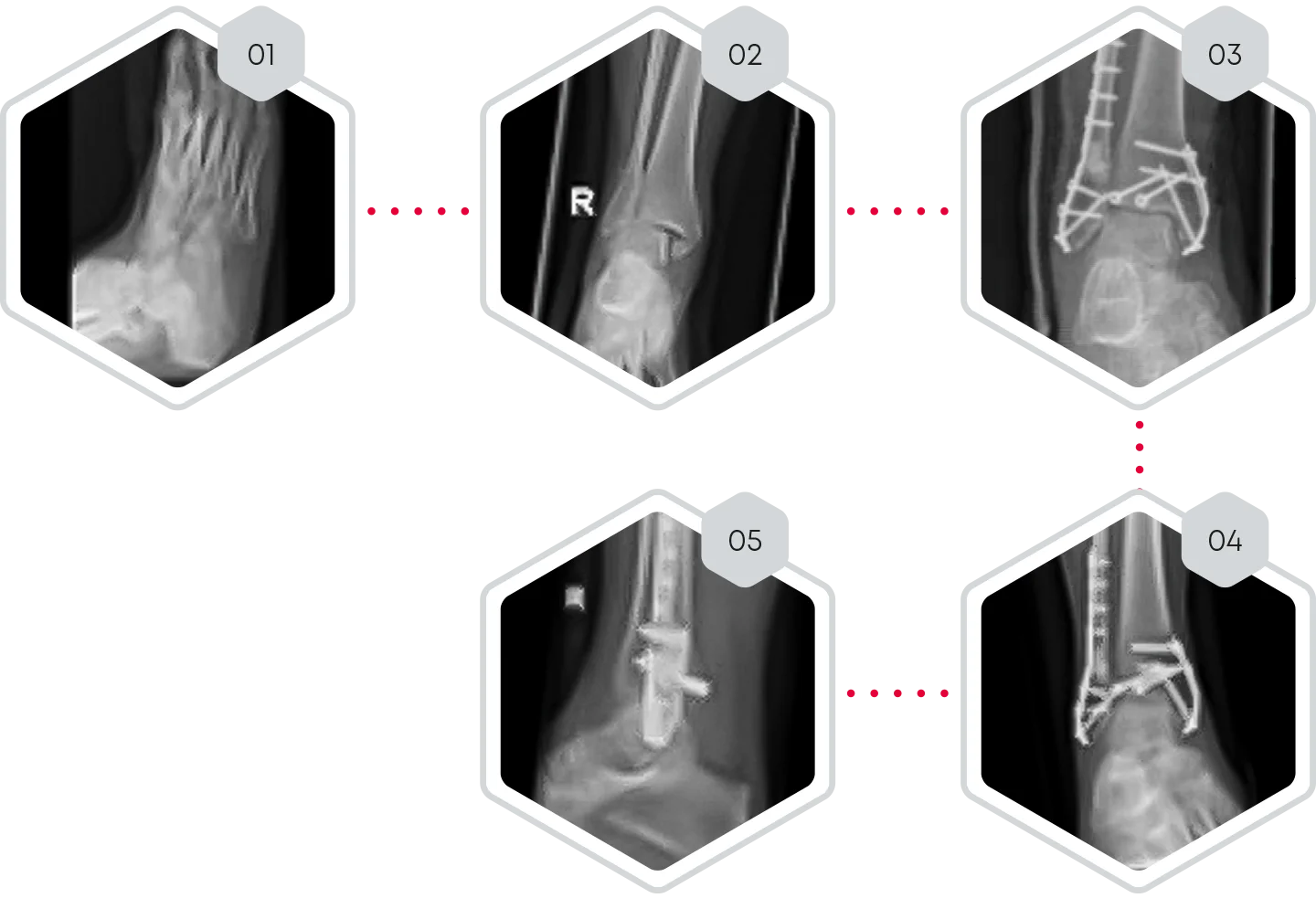
❯ 01-02 Pre-operative X-rays of ankle fracture type WEBER C with bony defect of distal fibula
❯ 03 Day 1 post-operative x-ray. Open reduction and filling of the fibula defect with CERASORB® CPC
❯ 04-05 10 weeks post- operative X-rays.
❯ Clinical follow-up.
❯ CERASORB® CPC was easy to handle during the operation
and allowed sufficient bone defect filling.
❯ 10 weeks post-operative, X-rays showed complete fracture healing
with beginning of osseous integration of CERASORB® CPC.
❯ CERASORB® CPC supports the defect through good osseous
integration and is gradually replaced by the newly formed bone.